Selling and Surviving in the New Pharma Landscape
Maria Whitman became the global head of ZS’s pharmaceutical and biotech practice in July 2021, having previously led the company’s global oncology and specialty vertical. In 2020, she steered the firm’s COVID-19 thought leadership workstream, and since 2019, she has served as chair of the practice council, focusing on the firm’s leadership in expertise, innovation and collaboration.
Pharma Commerce sat down with Maria recently for a wide-ranging chat on what she has been hearing from pharmaceutical and biotech companies, including the upheaval of the pharma business model and what it means for sales reps; the current skills gap in the marketplace; and how mega-mergers and big acquisitions will soon be back on the agenda.
Pharma Commerce: Looking at the changing pharma business model and the evolving definition of a pharma company itself, what are the operational implications of this from a sales rep’s point of view?


Maria Whitman

Maria Whitman: Between COVID economic pressures, the redefining of what innovation is, what we’re actually selling, and the advent of digital and AI, we have what I’d call a disaggregation of core competency. Historically, core competency for pharma is designing and developing products and then delivering them out in the market. Moving the earlier aspects of the value chain aside and focusing in on commercial, there is an intersection of a couple of things that are driving a very acute change on the ground for reps. One is that, instead of pushing information, there is now very much a dynamic push-and-pull, meaning you need to bring value that encourages a customer to engage with you, vs. pushing it to them in an in-office setting. In every other part of life, customer are becoming used to engaging ontheir terms as a citizen, no matter what industry you’re in. It is a general expectation that you as a company are thinking about who I am, and connecting to what I value, not to what you’re trying to push on me. This has lead to a significant focus on hyper-personalization in insight and execution around customers.
The second thing has been the evolution of digital as a mode of communication. We are very advanced now into this world of omnichannel, where pharma companies can deliver hyper-personalized experiences. But that requires more than just that capability; it requires a massive strategic shift in thinking about leveraging the capabilities to deliver in a way that best meets the customer needs and delivers on my intent. Companies need to take the leap to deploy omnichannel as a holistic strategy, not “I have reps and this digital stuff; how do I mesh it and get it out there?”
I also think that, from a talent perspective, there’s been a massive desegregation in terms of what is going to be successful in the future. It’s not the ability to relay information. It’s very much about sustaining a relationship that is continuing to move from telling you the benefits and features of a product to delivering a foundational experience. The next phase is being able to connect the dots to patient outcomes. How is what I’m doing—not just this singular brand, but the portfolio of products and services—serving patient outcomes more broadly than medicines outcomes?
It's a long way from what the ‘old school’ reps were doing. Are we looking at a new approach to talent in terms of the people pharma needs to recruit?
I think so. It’ll be dependent in part of what category we’re talking about. Medical affairs, for example, is much more confident in that virtual space. In fact, it’s encouraged a different level of peer-to-peer relationships. In global research ZS conducted in 2021, 70% of KOLs are comfortable with virtual engagements. There is a rise overall in medical affairs right now built on customer needs. Investments are not only in more medical face to face field, but medical communications, medical information and HEOR, and channels to facilitate medial exchange.
When it comes to sales reps, we are moving from in-person, relationship-centered, detail-aid delivery to needing individuals who can pull through a relationship and a continuous story across all of those channels at the right time with the right customer.
We did some sales rep capability research recently that showed there is a skills gap among 60% of reps today that are in the marketplace. The gaps are primarily categorized into four areas: solution specialists, adapters, networkers, and omnichannel. Can the rep solve an issue when it’s brought to them? Can they adapt to the format, the content, the moment, and the question that somebody is asking? Can they network appropriately and draw the right connections with the clients and within their own organization? And can they engage with clients in a synchronous way? I’ll tell you that more than 60% of reps are challenged by the first three, and at least 30% are really struggling on the fourth.
So, what do we believe needs to happen? One thing we’re going to see in the coming years is the traditional things that drove reps engagement, call planning, targeting, etc., giving way to AI-generated information of about what to do next. It’s already kind of there, of course. We’re already doing next-best intelligence, but even with that, how do you eliminate the idea that I have a call list and operate more on the basis of real-time information? All that will mean a lot of change. Companies will be looking for people who can engage more like people do in everyday life, who can maintain compliance, but also create a dialogue. In the past, pharma taught people to not do that, but to stay focused on the message in the format and order intended.
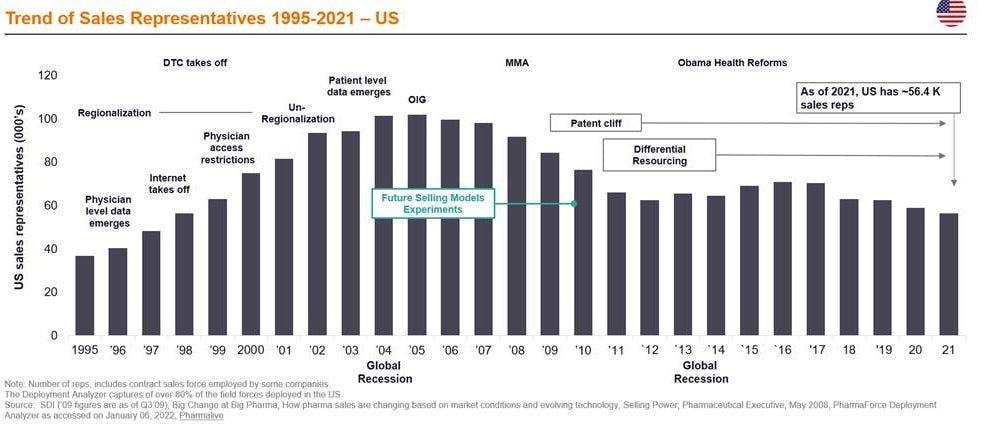
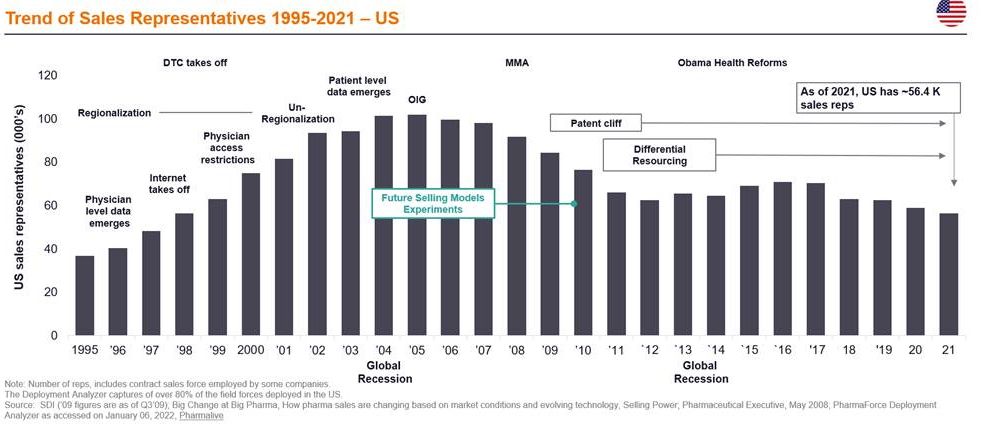
We’ve seen an overall reduction in rep numbers. How do you think this will continue?
From 2020 to 2021, rep numbers dropped by 5% and there have been a number of companies announcing that they’re going continue to scale down in this area. It does vary a little bit by specialty category, but companies are saying that they want 60% of their interactions to be virtual, on average. This is not surprising given that capacity was not well utilized during the beginning of COVID. The industry did rapidly make the transitions needed to virtual, but still about 25% of rep was not used.
Another implication that’s going to drive change is that, while pharma has been historically very brand-centric, going back to the concept of outcomes and being patient-led, portfolios are starting to change. Companies are thinking not just the brand and the asset, but the portfolio of impact. It’s about changing the dialogue around the impact a company is trying to have in a particular category, including services and solutions that address unmet needs—whether digital and connected health or patient navigation, for example, because that’s the value that pharma will be measured on in the future. That also creates a very different perspective on how you build the right volume of people in the market.

As you mentioned COVID there, could you talk a bit more about the role it’s played in boosting the patient-led model?
I think the velocity under which that change has now been realized is under reported. The fact is that 90% of Americans and 55% of Europeans consult “Dr. Google” before they even think about calling a doctor or engaging in some way with the health system. And they make choices driven by affordability, on their perceptions of what kind of care they’re going to get, and on their own assessment of the importance of taking that route versus continuing to go to work or doing all the other things they have to do. Patients are already making a significant volume of choice in that first level of engagement. The second thing is, as you look at the shift in disease areas, you can’t help but start to be patient-led. Look at diabetes. The marker of success is very rapidly moving away from reduction of A1C to detecting prediabetes and reversing it, or even bringing Type 2 diabetes into remission. If that is the goal, then pharma obviously has to change its focus on how it is serving that goal.
I’d also say that patient engagement, especially during COVID, became the mechanism by which information is exchanged. Over the previous 30 years, pharma spent 90% of its attention on the HCP. What I expect to see in the next two to three years is that at least 30 or 40% of that energy, if not more, going into patient engagement services and solutions, which also present valuable revenue streams for pharma. We did a study recently with 4,000 US citizens and a number of doctors on how digital has advanced patients’ ability to connect into health during the pandemic. It revealed that more than half of patients have a radically different experience with their doctors than the doctors think they do. More than 50% want a significant role in designing their care in the future. This pushes back into the concept of the patient saying “I want to change my engagement; I want to be more in control. If I’m not getting what I need, I’m not going to engage in the first place.”
In terms of this new model, what do you see in terms of company preparedness for it? Novartis said some time ago that they were becoming this digital healthcare company, as opposed to a pharma company. Do you see other companies following suit?
Let’s look at the digital angle first. I just did a Voice of the Customer of senior executives across the industry and it showed the majority of companies still don’t have a consistent definition of digital in their organizations. The majority of pharma companies have deployed digital as omnichannel solution. There is activity in AI-based discovery biomedical research and companies are asking how automation can add speed in both R&D and commercial. But broadly, no pharma company is close to approaching a digitally native organization. One of the big barriers is the enterprise data strategy capability to do it. We’re working with clients on building the foundations to achieve this, but the change management has to come from within.
Thinking about the new pharma model, it depends heavily on where a pharma company is now and where it is going. You have large pharma companies that have a very wide breadth portfolio of many things. You have other companies that are focused in a singular diseased area. The first decision driver as regards the future model is, “What level of focus am I going to have?” And is it going to be a product focus or, as I mentioned, a disease and outcomes focus? Question number two is, “What am I developing in that focus?” This is a challenge for both the internal organization and the field organization at the end of the day. We are seeing significant movement from singular assets with multiple indications because there are fewer blockbusters out there, to platform technologies that can produce many assets in as many categories as needed. The third thing is that what pharma is selling is changing. We know now that only 20% of a person’s health is based on genetics the other 80% comes from behavioral and environmental factors. Are companies able to step back and engage in different revenue models, beyond products and platforms? Can they develop clinical decision support from prevention all the way through to treatment? Can they offer surrounding services and solutions, whether that’s a nurse navigator or digital apps and technologies? Those key strategic decisions have to be made and companies have to decide, “Are we going to play by doing, or are we going to play by partnering?”
How long does pharma have to make these transformational changes, would you say?
Not very long. I say that because I’ve been watching very closely the reality of the patent cliff that’s coming. The top 10 biopharmas stand to lose $236 billion in the next eight years. About five will lose in the beginning and about five at closer to the end. Why is that relevant? It’s half of their worldwide revenues. I’ve looked out to 2025 on the basis of the pipelines they have behind them, and four companies still have more than 50% of their revenues at risk, even with their pipelines risk adjusted. Companies need to worry because even if they find ways to blunt the revenue curve (which with biologics, is still more possible) and fill the gaps, it’s going to have be with many more assets, many of which will need to be acquired at a time of high valuation and intensive competition to get to those assets and lead molecules. The technology that’s getting the most attention now, outside of pure oncology, is cell and gene therapy. Cell and gene therapies have so much scientific potential for cure, but the COGS and the margin profiles of these and global supply chain issues are challenging pharma very extensively on the investment to commercialize.
So, pharma is going to be facing some pretty staunch challenges, not only in replacing lost revenue, but bringing to market new innovation of different shapes and sizes, while sustaining the really high growth expectations that have come in the last few years. I think that means a couple of things. One is that executives will be asking, “Can we do more with data? Can we do more with AI to drive decisions and automate decisions? Can we reduce risk in R&D and in corporate strategy selection of partnerships and assets? And can we reduce risk and speed up decision making through better analytics?” The other factor is going to be cuts in selling, general, and administrative (SG&A) expenses. This is where I think reps and others will be affected. I have seen reports that estimate that $32 billion needs to be cut from SG&A in the biggest pharma companies by 2030. On average, that is $3 billion a year in expenses. That says we’re going to have to see very different organizations in the future. While we’re seeing the softening of M&A activity in 2022, I think that will be a short-lived phenomenon. A key way forward for some of these big pharma companies is bolt-ons, mergers and big acquisitions in the future.

















